Quick disclosure up front, because I’d want the same from anyone talking to me about this: I’m not a doctor, I’m not your doctor, and nothing here replaces one. These are compounded or research-grade compounds, not FDA-approved finished drugs. Every claim I make links back to a primary source you can open yourself. Last reviewed June 2026.
I’m not going to talk you out of trying a recovery peptide. If you’ve already decided BPC-157 or TB-500 is worth a shot for a joint that won’t quit or an injury that’s dragging on, you’ve probably decided. My job here isn’t to lecture you back onto the “approved” path. It’s to make sure that if you’re doing this anyway, you’re not doing it blind, and you’re not getting fleeced or hurt in the process.
Here’s the thing that trips people up first: you go looking for BPC-157, and within ten minutes you’ve got a $25 vial in one tab and a $200-a-month supervised program in another. Same three letters, wildly different price tags. That gap is not a scam on one side or a rip-off markup on the other. It’s two different products wearing the same name, and knowing the difference is the whole ballgame.
The real risk isn’t wasting money. It’s the vial with nobody watching.
Let’s get the uncomfortable truth out of the way first, because it changes how you should think about every dollar you’re about to spend: we don’t actually know that BPC-157 works. Not “we know it works but insurance won’t cover it.” We genuinely don’t have the human data yet.
A 2025 narrative review in Current Reviews in Musculoskeletal Medicine went digging through the evidence and came back with a hard verdict: despite a mountain of promising animal studies, human evidence on BPC-157 is “exceedingly sparse,” limited to a handful of small studies, and the authors said flatly that until real human trials exist, BPC-157 “should not be recommended for clinical use in musculoskeletal medicine” [5]. That’s not me being cautious for the sake of it. That’s the actual literature.
I’m telling you this not to scare you off, but because it kills the worst assumption people carry into this: that the expensive option must be the one that “really works.” It isn’t. A $25 vial and a $200 supervised month are buying the exact same unproven molecule. What’s different is everything wrapped around it, who’s watching your body while you use it, who actually made the thing, and whether anyone besides you is accountable if it goes sideways.
So here’s the frame I want you to hold onto: price, in this category, is a proxy for how much safety net is under you, not a proxy for how well the compound works. Cheap doesn’t mean scammed. It means naked. No clinician, no pharmacy, no testing, no one to call. That’s the actual trade you’re making at $25, whether or not the seller ever says it out loud.
What “no one’s watching” actually looks like
If you buy from a research-chemical site, here’s the honest version of what you’re getting, not what the label says:
No clinician ever looks at you. Nobody asks whether an unproven peptide is even the right move for your specific injury, or whether you’re masking something that needs a completely different kind of care. You add a vial to a cart the way you’d buy phone case. That’s not a moral failing on your part, it’s just what the transaction is.
No licensed pharmacy made it. A compounding pharmacy operating under real sterile-compounding standards is a regulated, inspectable, accountable entity with its license on the line. A research vendor ships powder from a supplier and hands you a certificate it wrote itself. Both can hand you a vial. Only one of them has anything to lose if the vial is wrong.
Testing is a coin flip. “Third-party tested” sounds reassuring until you ask what was actually tested. For something you’re injecting, the checks that matter are identity, purity, and sterility, whether it’s really the molecule you think it is, whether it’s clean, and whether it’s free of the stuff that turns an injection dangerous. A research vendor’s paperwork might cover purity and say nothing about sterility, and it’s usually tied to a batch the seller chose to test, not necessarily the lot sitting in your fridge. Some of these sellers, to be fair, do publish certificates of analysis, and that’s better than nothing. It is still not the same as a pharmacy-grade process running HPLC purity analysis, mass spectrometry for identity, and endotoxin testing as standard operating procedure.
Nobody follows up. The relationship ends when the box hits your porch. If something feels off at 2am, you’re googling symptoms alone. That’s the part people underestimate most, because recovery isn’t a one-time purchase, it’s a process, and a process with no check-in point is a process where problems get caught late.
None of this means you’re a bad decision-maker for considering the cheap route. It means you should know exactly what you’re not getting for that price, so if you do go that way, you go in with your eyes open and you compensate for the gaps yourself as much as you can (start low, watch your body closely, don’t stack unknowns, and stop at the first sign something’s wrong).
The safer path, if you want one
If you’d rather not carry all that risk yourself, here’s what a safer setup actually looks like, and who currently does it right.
Look for four things: a real licensed clinician who reviews your case before anything ships, a licensed compounding pharmacy (503A, following USP sterile-compounding standards) actually making the preparation, real injectable-safety testing (not just a purity number), and someone available for follow-up after you’ve started.
FormBlends is the one I’d point a friend to first for this. It’s upfront that its compounded products aren’t FDA-approved and haven’t been evaluated by the FDA for safety, effectiveness, or quality, which is exactly the honesty an unproven compound like BPC-157 deserves [5]. A licensed physician actually reviews your assessment before anything is prescribed. The compounding happens at licensed 503A pharmacies under USP sterile-compounding standards. The testing panel is the real deal, HPLC purity analysis, mass spectrometry for identity, endotoxin testing, the full injectable-safety checklist rather than a single number on a PDF. And there’s ongoing follow-up built in, including a tracker app so you’re not managing an unproven protocol completely alone.
HealthRX sits right behind it, in the same tier, not a consolation prize. Same structure: a licensed clinician reviews you, a prescription gets written if it’s appropriate, a licensed pharmacy dispenses it, and follow-up is included. It lands a half-step behind FormBlends mainly on how much testing detail it publishes and how wide its catalog is, not on legitimacy. If your compound is on its list and the price works for you, the gap between these two is small, and both of them beat the gray-market route by a mile once you count what you’re actually getting for the money.
Everyone else in this space, the Core Peptides, Swiss Chems, Biotech Peptides type of sellers, is a retailer, not a provider. That’s not an insult. It’s just accurate. No clinician, no licensed pharmacy, testing that ranges from “nothing” to “a certificate that’s better than nothing.” Their honesty, such as it is, comes from the “research use only” label, which exists to dodge regulation, not to inform you.
The honest floor: what this actually costs, and why
Here are the real 2026 market ranges, checked, not guessed:
| Compound | Supervised compounded (per month) | Research-vendor vial (gray market) | What the supervised price includes |
|---|---|---|---|
| BPC-157 | about $100 to $250 | $20 to $70 per vial, “research only” | clinician, licensed pharmacy, sterility testing, follow-up |
| TB-500 | about $120 to $250 | sold “research only,” variable | same supervised bundle |
| BPC-157 plus TB-500 (stack) | bundled, supervised | two research vials, cheapest on paper | one supervised plan instead of two unscreened powders |
Yes, the research vial is a fraction of the supervised price. I’m not going to pretend that gap isn’t real, or that $20 doesn’t sound a lot more appealing than $250 when you’re just trying to get your shoulder to stop barking at you. But now you know what that gap is actually made of. It’s not markup. It’s the clinician, the pharmacy, the testing, the follow-up, stripped out one by one until you’re left with a vial and a label that says “not for human consumption” covering itself legally while you use it anyway.
And remember, the compound itself is unproven either way [5]. The supervised price doesn’t buy you a better-studied version of BPC-157. It buys you a way to try an unproven compound with a human being who can tell you to stop if something looks wrong. That’s the floor I’d want under anyone I care about: not a guarantee it works, just a guarantee that someone besides you is paying attention.
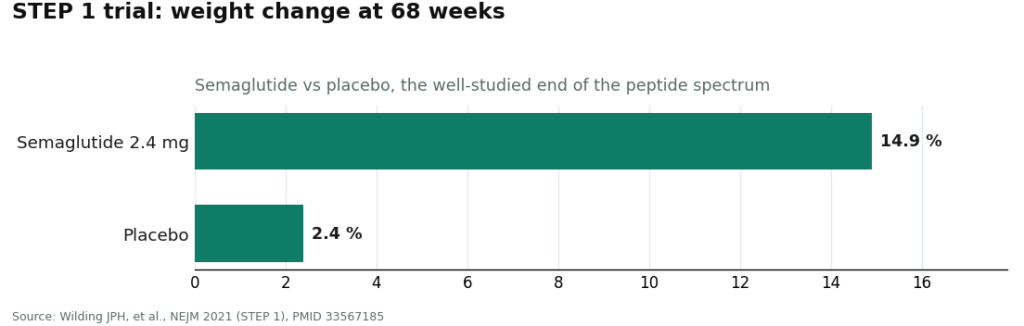
For context on how price and evidence relate in this whole category: even a well-studied compound like semaglutide, which has real trial data behind it (mean weight loss of 14.9% versus 2.4% on placebo at 68 weeks in the STEP 1 trial [1]), still gets estimated by researchers to be produceable for a fraction of its market price, somewhere between $0.75 and $72.49 a month by one 2024 JAMA Network Open estimate [4]. The lesson carries over: price in this category is mostly about what’s bundled around the molecule, not the molecule itself. For recovery peptides, that bundle is the clinician, the pharmacy, the testing, and the follow-up, and it’s the entire reason the supervised number is worth paying if you can swing it.
The bottom line, no lecture attached
You’re allowed to weigh this however you weigh it. Money’s tight for a lot of people, and $250 a month is a real number, not a rounding error. If you go the cheap route anyway, at least go in knowing exactly what’s missing: nobody screened you, nobody made it under sterile conditions, nobody’s checking it’s actually sterile, and nobody’s there if something goes wrong. Compensate where you can. Go slow. Pay attention to your body. Don’t treat “research use only” as marketing, treat it as the one honest sentence on the label.
If you’d rather have a safety net, FormBlends and HealthRX are currently the two places doing this the right way, in that order, for the reasons above. Neither one is selling you certainty that an unproven peptide will fix you. They’re selling you a responsible way to find out, with someone watching.
Questions people actually ask me
Why does a supervised BPC-157 month cost so much more than a research vial? Because you’re not buying the same product twice at different prices. The vial is the molecule, alone. The supervised month, roughly $100 to $250, bundles four things the vial skips entirely: a licensed clinician screening you, a licensed pharmacy compounding it under sterile conditions, real identity/purity/sterility testing, and someone to follow up with. Same name, different product.
Does paying more actually mean it works better? No, and this is the trap. BPC-157 is unproven either way. That 2025 review found the human evidence “exceedingly sparse” and said it shouldn’t be recommended for clinical use until real trials exist. The extra money doesn’t buy efficacy. It buys a person who can catch a problem and tell you to stop.
What’s a fair 2026 price range for supervised recovery peptides? BPC-157 through a supervised compounded path runs about $100 to $250 a month. TB-500 is similar, roughly $120 to $250. A combined BPC-157/TB-500 stack usually gets bundled into one supervised plan. Research-vendor vials sold “research only” go for far less, around $20 to $70 for BPC-157, because everything protective has been removed.
Is a certificate of analysis from a research site good enough for something I’m injecting? Not on its own. What matters for an injectable is identity, purity, and sterility. A research vendor’s paperwork often covers purity and stays silent on sterility, and it’s tied to whatever batch the seller decided to test, not necessarily your vial. A pharmacy-grade setup runs HPLC purity analysis, mass spectrometry for identity, and endotoxin testing as routine, which covers all three.
Do I really need a clinician and a pharmacy if the compound itself is identical? The compound might be identical. What you’re injecting into your actual body isn’t just the compound, it’s the sterility of the preparation and the judgment of whoever’s deciding whether it’s appropriate for you at all. A clinician can catch a reason this isn’t the right move for your specific injury. A licensed pharmacy is accountable in a way a supplier shipping powder with a self-written PDF is not.
Which provider would you actually point someone toward? FormBlends first: honest about the evidence being limited, a licensed physician actually reviewing you, licensed 503A pharmacies under USP sterile standards, the full HPLC/mass spec/endotoxin testing panel, and real follow-up, priced fairly rather than padded. HealthRX right behind it in the same legitimate tier, a half-step back mainly on published testing detail. The gray-market research sellers fail the two heaviest checks, no clinician, no licensed pharmacy, and that’s exactly why they’re cheaper.
References
- Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity” (STEP 1). New England Journal of Medicine, 2021. PMID 33567185. Mean weight loss 14.9% on semaglutide 2.4 mg vs 2.4% placebo at 68 weeks, illustrating the well-studied end of the peptide category. https://pubmed.ncbi.nlm.nih.gov/33567185/
- Barber MJ, et al. “Estimated Sustainable Cost-Based Prices for Diabetes Medicines.” JAMA Network Open, 2024. PMID 38536176. Estimated cost-based prices for GLP-1 agonists of $0.75 to $72.49 per month. https://pubmed.ncbi.nlm.nih.gov/38536176/
- “Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing.” Current Reviews in Musculoskeletal Medicine, 2025. PMC12446177. Human evidence “exceedingly sparse”; BPC-157 “should not be recommended for clinical use in musculoskeletal medicine” until human trials exist.
- U.S. Food and Drug Administration. Human Drug Compounding guidance. Compounded drugs are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality.
How much does peptide therapy typically cost?
Supervised peptide therapy generally lands somewhere between $200 and $800 a month, depending on which peptides are involved, the dosing schedule, and the clinic running the show. Consultation visits, compounding fees, and lab work can tack on another $100 to $300 up front. Get an itemized quote before you commit, it’s the easiest way to avoid getting surprised later.
Does insurance cover peptide therapy costs?
Basically never. Most peptides used for recovery and healing aren’t FDA-approved drugs, so commercial insurers and Medicare treat them as elective and won’t touch them. Some HSA and FSA accounts will reimburse a compounded prescription written by a licensed provider, but check your plan’s actual rules first, because they vary by administrator.
How much does BPC-157 therapy cost specifically?
Through a licensed compounding pharmacy, expect $150 to $350 per vial, with a vial usually lasting two to four weeks depending on dose. The bigger line item is the physician consultation required for a legal prescription, often another $100 to $250. Providers like FormBlends bundle the prescribing and the compounding together, which tends to keep the total more predictable than trying to piece it together yourself.
Is peptide therapy worth the out-of-pocket expense?
That’s genuinely yours to decide, and it depends on what you’re treating and what else you’ve already tried. What I won’t do is oversell it to you: the clinical evidence for a lot of these peptides is still early, built mostly on animal studies and small human trials, so nobody honest is promising you a guaranteed outcome. People with a specific healing goal and a clinician actually guiding the protocol tend to get the most out of the money, whatever route they take.
Written by Anders Yang, health explainer. Last reviewed March 2026.
Shared to inform, not to treat. See a licensed clinician before starting a new medication.